

Paediatric closed claims – Opportunities for learning



Aim
To review all closed claims pertaining to Paediatrics in 2014, and identify opportunities for learning.
Method
A retrospective, one year review of all closed claims, nationally, pertaining to Paediatrics was conducted. A report was generated using the NIMS (National Incident Management System) and a search carried out using the term “paediatrics” and age band “0-17 years”.
Results
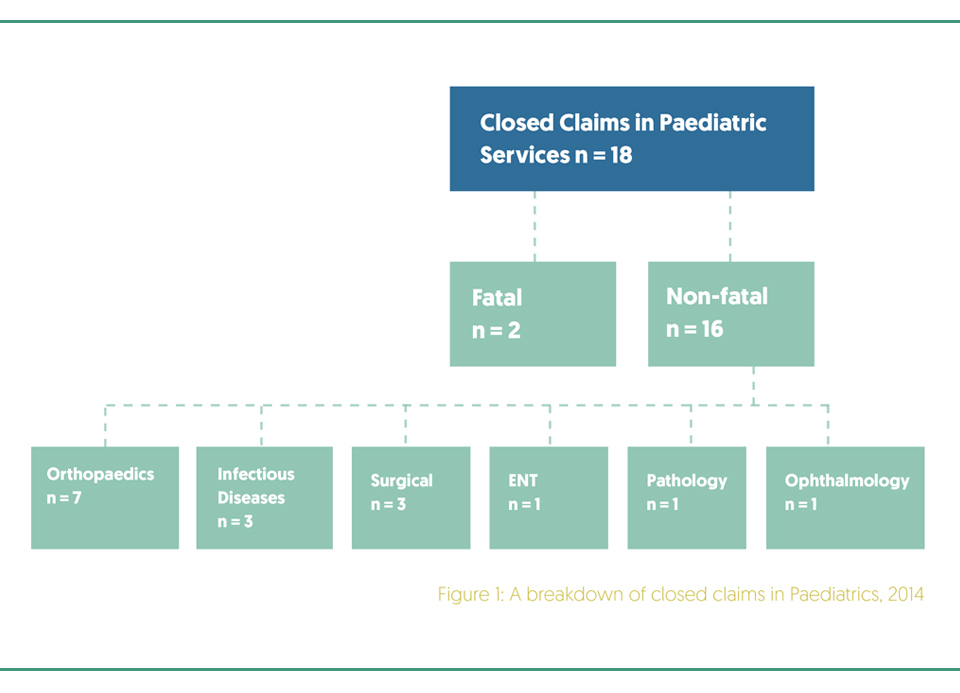
Of the eighteen closed claims analysed, twelve (66.7%) involved males. Regarding age, eleven (61.1%) involved children less than five years of age. Two (11.1%) claims pertained to fatalities. (Figure 1).
Of the two fatal claims, one related to a five month old boy with bacterial meningitis who, on initial presentation, was diagnosed with a viral infection. He later re-presented and a diagnosis of Streptococcus pneumoniae meningitis was made. Despite appropriate treatment the infant subsequently died.
The second fatal claim related to an 18 month old, ex premature infant (26 weeks gestation) who presented to the Emergency Department with respiratory symptoms. A diagnosis of bronchiolitis was made. Upon clinical deterioration, the child underwent treatment with intravenous antibiotics, was intubated, ventilated, and transferred to the adult intensive care unit (ICU) while awaiting transport to a tertiary paediatric ICU. During the ICU stay, the endotracheal tube became blocked and dislodged. The infant suffered a cardiac arrest and, despite resuscitation, care was withdrawn two weeks later due to severe hypoxia and confirmed brain death.
Regarding the non-fatal closed claims (n=16), multiple specialities were identified of which the most common pertained to Orthopaedics (n=7), Infectious Diseases (n=3) and Surgical (n=3). There was one claim each in the specialities of Otolaryngology / Ear, Nose and Throat (ENT), Ophthalmology and Pathology.
Regarding Orthopaedics (n=7), the mean age was 9.4 years, ranging from 8 months to 16 years, of which five cases pertained to males. Two claims were related to fractures, both resulting from trauma: fall from a trampoline and a bouncy castle. A delayed diagnosis of slipped upper femoral epiphysis in a female patient resulted in chronic pain, restricted joint movement and the likely need for further surgery. A systems error resulted in a delayed diagnosis of developmental dysplasia of the hip in an infant with a known family history for this condition.
The category with the most significant clinical outcomes, though not the most common, was Infectious Diseases (n=4, 22.2%). One case resulted in a fatality while another involved a missed septic arthritis, secondary to Haemophilus influenza b septicaemia involving several leg discrepancy length corrective surgeries.
Three cases pertained to surgery. One pertained to an upper labial frenulum release but the surgery performed was lingual frenulum release. Another case related to a missed anal atresia in a new-born infant. The infant was re-admitted within 24 hours and required a laparotomy and colostomy.
Suggested opportunities for learning:
- Specific training and education in Paediatric medical and surgical emergencies (diagnosis, and management) and Paediatric Orthopaedic conditions (presentation, radiological findings and management) particularly for junior doctors, early in post or prior to commencement in post if possible (e–learning).
- Early escalation to senior colleague if any doubt regarding diagnosis and / or management plan.
- Clear, timed documentation in healthcare records regarding diagnosis and management.
References available on request.
Article By: Deirdre Walsh, Clinical Risk Adviser, State Claims Agency